Hysterectomy, Minor surgical treatment
In the past, many women underwent hysterectomy, a major operation, even though they didn’t have any significant or serious disease within the uterus. In recent years surgical procedures have been developed in which the endometrium (the uterine lining) is removed or destroyed, leaving the remainder of the uterus and the ovaries undisturbed. This is known as endometrial ablation. This chapter also describes alternative surgical methods of treatment for endometriosis and uterine fibroids.
Endometrial ablation
There are several ways in which this can be performed and they all avoid the need for a surgical incision. The methods used vary in cost and complexity, and the method or methods available in your hospital will depend on the equipment available and the preferences of local gynaecologists.
Most endometrial ablations are carried out under a general anaesthetic although, in some hospitals, it is available under a local anaesthetic. All procedures are carried out via the vagina, by passage of instruments into the cavity of the uterus through the cervix.
Older (First Generation) methods of endometrial ablation
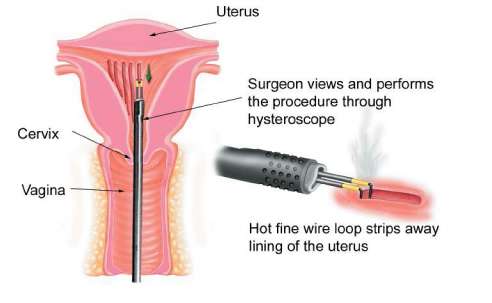
Endometrial resection
Endometrial resection and TCRE (transcervical resection of the endometrium) are terms used to describe the removal of the endometrium (uterine lining) in strips using a fine wire loop through which an electric current is passed (electrodiathermy). This heats up and coagulates the muscle wall of the uterus at the same time as it strips away the lining, thus reducing the risk of haemorrhage.
The wire loop is inserted down the side channel of a hysteroscope so that the surgeon can watch the procedure on a screen. The uterine cavity is continuously flushed through with fluid to open it up and give a good view while simultaneously washing out blood and lining tissue and cooling the uterus down. Endometrial resection is now much less popular than other methods of ablation because it is more difficult to perform and carries a slightly greater risk of complications than the newer methods (see below).
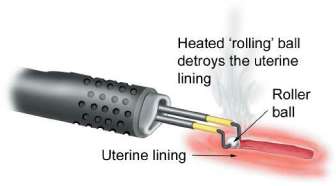
Roller ball endometrial ablation
This is similar to endometrial resection in that it uses heat generated by electricity (electrodiathermy) but the difference is that the uterine lining is destroyed by contact with the ball which is rolled slowly over the surface. Like endometrial resection, the procedure is done using a hysteroscope with constant fluid irrigation.
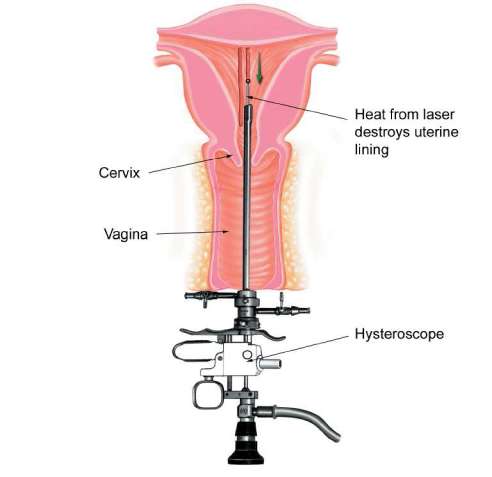
Laser endometrial ablation
This destroys the endometrium using heat generated by a laser. The laser beam is passed down the side arm of a hysteroscope and guided by the surgeon over the uterine lining. The laser is in many ways ideal for this task but has the disadvantage of being very expensive and beyond the price range of most NHS hospitals.
Complications
First generation methods of endometrial ablation are very effective but do carry some risks. As with all operations these include difficulties resulting from the use of the anaesthetic, excessive bleeding (haemorrhage) and infection. These complications are less likely following all methods of endometrial ablation than they are after a hysterectomy.
Other complications that arise only after endometrial ablation or resection are uterine perforation (see below) and absorbtion of the irrigation fluid into the circulation which, if excessive, can put a strain on the heart and circulation – a condition known as fluid overload. Between two and six per cent of first generation endometrial ablation operations have serious complications and the risk of complications is slightly higher with endometrial resection than with other methods. However in hospital that have carried out these procedures for a number of years they are generally very safe and effective.
Newer (Second Generation) methods of endometrial ablation
Endometrial resection and the other first generaton methods described above, although much simpler than hysterectomy, are time consuming to perform, difficult to learn and not available in all hospitals. Recently several newer methods have become available, based on developments in technology, each using a different way of delivering heat to the uterine cavity in order to destroy the endometrium. They do not involve fluid irrigation and are much quicker to perform.
Results of clinical trials show that they are equally effective and, most importantly, safer than the first generation methods and endometrial ablation is now available in most hospitals. They are performed in conjunction with hysteroscopy or ultrasound so that the gynaecologist can check that the instrument is placed correctly in the cavity of the uterus before activating the heat source.
Microwave endometrial ablation (MEA)
A probe of suitable size is inserted into the cavity of the uterus, the heat source is triggered and the probe is gradually moved around the cavity for the length of time needed to destroy the endometrium. It is suitable for use where there are small fibroids but may not be suitable for some women who have had one or more caesarean section births because this may result in thinning of the uterine wall and a greater risk of damage due to perforation. If you have had one or more caesareans in the past, an ultrasound scan will be done to measure the thickness of the wall to see if you are suitable for MEA.

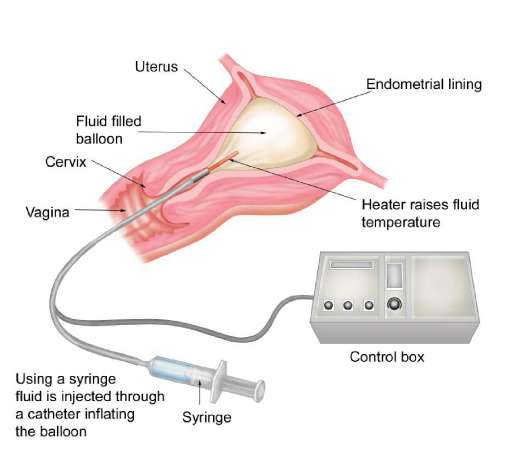
Thermal balloon ablation
A small balloon is inserted into the cavity of the uterus and filled with fluid so that it fits the shape of the cavity exactly. It is then heated to a temperature sufficient to destroy the endometrium over a set time. This method is not suitable for women who have fibroids within the cavity of the uterus. It is probebly the safest of all the methods of endometrial ablation and is more suitable than other methods for use under a local, rather than a general, anaesthetic.
Other methods
Other methods are being developed all the time. You may read about one of these in a newspaper or magazine, or even on the Internet, only to find that it is not available locally. This is because new treatments have to be thoroughly tested and compared with existing methods before they can be introduced more widely. Some hospitals will prefer existing methods; others may be involved in testing out one of the newer methods.
Complications of second generation endometrial ablation
These methods are safer than the first generaton methods because they do not require fluid irrigation and the risk of haemorrhage is much lower. However technical problems with the equipment may occur, resulting in delay and sometimes rescheduling of the treatment if the problem can’t be sorted out right away.
A rare but potentially serious complication is perforation of the uterine wall by the instrument used to heat the uterine lining. If this is recognised immediately the treatment has to be abandoned. If the perforation isn’t spotted immediately and the treatment goes ahead, this can result in damage to nearby structures, including the intestines and large blood vessels, and emergency surgery to repair the damage is then required. Fortunately this is a very rare occurrence.
Other side effects of endometrial ablation
It is usual to experience cramping period-like pain for a few hours after the procedure and pain killers are routinely prescribed both before and after. It is also normal to experience a vaginal discharge for up to two or even four weeks afterwards. This is initially blood stained, then gets progressively more watery. If the discharge becomes offensive or if you develop a temperature and feel unwell this may be a sign that you have developed an infection. This occurs in 2-4% of women after endometrial ablation. You must contact your doctor as a course of antbiotics may be required.
Drug treatment before endometrial ablation
During the menstrual cycle, the uterine lining gradually grows and thickens in preparation for possible pregnancy as described on page x. The older (first generation) methods of ablation are more difficult to carry out and do not work so well if the endometrium is very thick . If these methods are used, it is usual to prescribe drugs to thin the lining in preparation for surgery. Thes drugs – usually a GnRH analogue or danazol – are prescribed for around four weeks before surgery. With the newer second generation methods, these drugs are less often prescribed.
The advantages of endometrial ablation
Although most endometrial ablation operations are carried out under general, rather than local, anaesthetic, they are performed as a day case procedure with no overnight hospital stay and recovery is considerably faster than after a hysterectomy. You will be able to take up your normal domestic activities after a few days and go back to work within one to two weeks – considerably less than the recovery time needed after a hysterectomy!
How successful is endometrial ablation?
In the short term, endometrial ablation has many advantages over hysterectomy but, unlike hysterectomy, it does not guarantee to stop all menstrual bleeding in the future. Survey results indicate that, two to three years after the operation, around 20 per cent of women have no menstrual bleeding and 50 to 60 per cent have reduced bleeding, but up to 25 per cent find that there is no improvement or an actual worsening. Longer-term follow-up indicates that over two-thirds of women treated with endometrial ablation are satisfied with the results and avoid hysterectomy. Women who respond well initially but whose heavy bleeding gradually returns may be treated successfully by a second endometrial ablation procedure. This is more likely to be required if you are under the age of 40 when you are first treated.
Is endometrial ablation right for you?
If you have completed your family and are seeking relief of heavy bleeding, do not suffer much menstrual discomfort and wish to avoid major surgery, endometrial ablation is an option well worth considering. However, you should always try medical treatment first.
This form of treatment is not suitable for women who may want to have children in the future. The procedure reduces fertility and, although some women have become pregnant after endometrial ablation, there is a very high risk of miscarriage and later complications.
- Very painful periods may not be relieved after endometrial ablation.
- Irregular bleeding may not improve after endometrial ablation.
- This type of treatment is not usually recommended for women with a uterus containing large fibroids (see below).
You should be aware that insertion of an IUS may be as effective as endometrial ablation, is more likely to relieve period pain, preserves fertility and avoids the potential risks of surgery.
Treating uterine fibroids
If medical treatment or endometrial ablation has failed or is not suitable, there are two other procedures which you may be offered which do not involve removing the uterus itself. These will not be appropriate for everyone.
Myomectomy
If you have not had children or want to have more in the future, it may be possible to remove the fibroids and preserve the uterus – an operation known as myomectomy. This is not easy to do from the surgeon’s point of view, particularly if there are several fibroids, and in some cases they may be very numerous. It is normally done by open surgery unless the fibroids are within the uterine cavity (see below). Laparoscopic (keyhole) methods may be used in some very specialised hospitals.
An operation to remove large fibroids may be complicated by heavy bleeding, so that a blood transfusion is necessary. In extreme cases, an emergency hysterectomy may have to be done, but this is fortunately rare. After a myomectomy, there is no guarantee that you can still become pregnant or that heavy bleeding will be cured and there is still a chance that further fibroids will grow in the future.
Is myomectomy right for you?
For the reasons outlined above, it does not make sense to opt for a myomectomy rather than a hysterectomy unless you are anxious to retain your uterus so that you can have children at some time in the future. However, if you have strong objections to hysterectomy for personal or cultural reasons, most gynaecologists will be sympathetic, provided that you fully understand the risks and limitations.
An operation to remove fibroids should be done only if the fibroids are causing symptoms such as pressure or heavy bleeding, not just because they’re there. Rarely, fibroids may be a cause of recurrent miscarriages, in which case they should be removed. However, most women with fibroids who conceive go on to have successful pregnancies. Similarly fibroids do not usually cause infertility although they are more common in women who have not had children.
Hysteroscopic myomectomy
Some women have fibroids that are situated within the uterine cavity, so-called submucous fibroids. If so, it may be possible to remove them with the aid of a hysteroscope, using methods similar to those described above. However, it is best for such procedures to be carried out in a hospital that specialises in hysteroscopic surgery because removal of fibroids in this way is difficult and requires considerable experience.
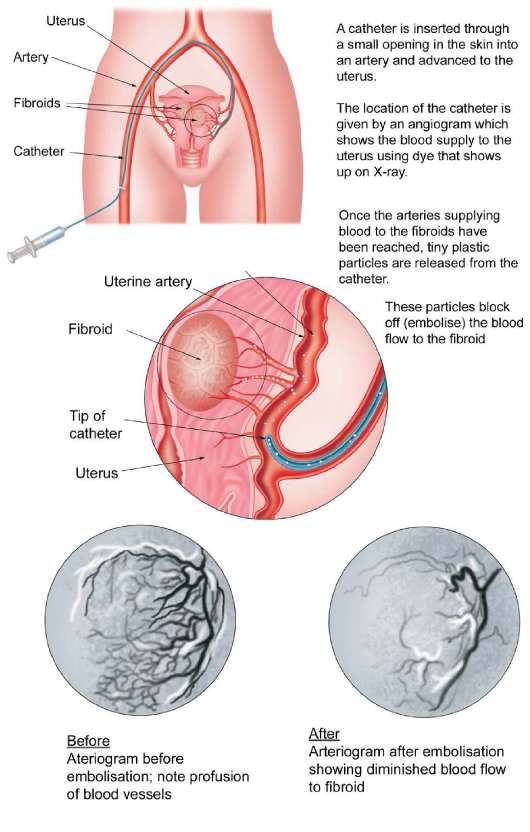
Fibroid embolisation
This is a new treatment that does not involve a surgical scar or a general anaesthetic. It is done by a radiologist and involves the use of X-rays. These show up the blood supply to the uterus (uterine arteries)by dye injected through a very fine plastic tube inserted into one or both groins.
Once the arteries (blood vessels) supplying the fibroids have been located, a special material is injected that blocks off (embolises) the blood supply. Initially, this causes as much pain as an operation. This is usually treated by an infusion of a strong pain killer such as morphine and it is necessary to stay in hospital for one or two days. Following embolisation most women are able to return to work within two weeks.
How successful is it?
Embolisation results in gradual shrinkage of the fibroids by up to 60% over the first year after treatment but they do not disappear altogether. Preliminary results suggest that the procedure relieves symptoms of heavy bleeding and pelvic pressure in around 80% of women but the long-term success of the treatment is not known. If the fibroids are very large or numerous, a 60% shrinkage may still leave you with symptoms of discomfort or pressure.
Are there any risks?
Following the procedure some women feel feverish and develop flu-like symptoms which settle within a few days. Rarely these symptoms persist due to the development of infection in the uterus. In very severe cases (around one per cent), this may necessitate a hysterectomy.
The main problem, experienced by up to one third of women, is a vaginal discharge which in some cases can persist for several weeks. There is also a very small risk of developing an early menopause. This would be a disaster if you plan to have children. However most women who have become menopausal immediately after embolisation have been over the age of 45. Overall the procedure seems to carry a low risk of complications and certainly fewer complications than hysterectomy or myomectomy.
Is embolisation right for me?
The most effective cure for fibroids is hysterectomy but this involves major surgery and loss of fertility. If you are approaching the age of the menopause and medical treatment is not appropriate or has been unsuccessful, embolisation is a sensible alternative to hysterectomy. It is also a realistic alternative for younger women who wish to avoid surgery.
The effects of the treatment on fertility are not known. Only a relatively small number of women have had pregnancies after fibroid embolisation and although the outcome has generally been successful, embolisation may not be recommended to women who plan to have children in the future unless their symptoms are very severe or the only other treatment option would be a hysterectomy.
Not all fibroids are suitable for embolisation and it is usual to assess suitability by performing a more detailed scan, known as an MRI scan, before any arrangements are made. Occasionally the procedure cannot be completed due to technical problems. Embolisation is not available in all hospitals and if you are keen to have this procedure you may need to be prepared to travel.
Treating Endometriosis
The diagnosis of endometriosis is usually made by laparoscopy and some gynaecologists will offer to treat small areas of endometriosis while they’re doing the diagnostic laparoscopy operation. This can be done using electrodiathermy (direct heat generated by electrical energy), by laser or by other similar methods.
If the endometriosis is more extensive, a second operation may be required to remove areas of endometriosis, possibly after a course of treatment with one of the drugs described on page xx. Endometriosis that has resulted in the formation of ovarian cysts containing altered blood (endometriomas or chocolate cysts) usually requires surgical treatment, and this is best done by laparoscopy rather than by open surgery, unless the cysts are very large. Surgery may be particularly beneficial for women who are trying to conceive a baby as hormonal treatment would not be suitable in this situation.
The disadvantage of surgical as opposed to medical treatment to relieve the symptoms of endometriosis is that not all areas of endometriosis are visible and thus the surgery may not relieve the discomfort altogether. Often a combination of medical and surgical treatment is the most effective. For women with severe endometriosis who want children, in vitro fertilisation (IVF) may be the best option and this can be combined with spells of medical treatment to relieve symptoms in between cycles of IVF.
Symptoms of endometriosis clear up during pregnancy and may be considerably improved thereafter, although a successful pregnancy does not guarantee a long-term cure of endometriosis
KEY POINTS
-
Endometrial ablation (removal or destruction of the uterine lining) is helpful in up to 70 per cent of women with heavy periods, but rarely stops bleeding altogether
-
Endometrial ablation is not suitable for women who have not completed their families and may not relieve pelvic pain
-
Endometriosis can be treated surgically without removal of the uterus or ovaries, but symptom relief may be only temporary
-
Myomectomy is an operation to remove fibroids that preserves the uterus in women who hope to have children
-
Embolisation is a new non-surgical treatment for fibroids which seems promising in the short term but its long term effectiveness is not yet known