Hysterectomy and your ovaries
Removal of the ovaries is not an automatic part of most hysterectomies, although it can be done at the same time and through the same surgical incision (scar). This should never be seen as a matter of convenience, just because you are having an operation done anyway. The question of whether your ovaries should be removed is very important and must be given very careful and separate consideration.
There will be some situations – for example, the treatment of endometriosis or certain forms of cancer – where removal of the ovaries is an important part of the treatment of the underlying problem. This does not apply to most hysterectomies carried out for the treatment of fibroids or menstrual problems.
What your ovaries do
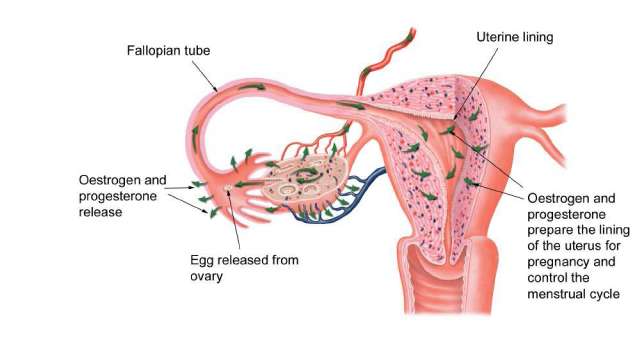
The main function of your ovaries is the monthly release of eggs to enable you to conceive a baby. The ovaries also produce the two hormones, oestrogen and progesterone, which prepare the lining of the uterus for pregnancy and control the menstrual cycle. Thus, if you are certain that you have had all the children you want, you may feel that your ovaries are no longer required. This is a long way from the truth. The hormone oestrogen produced by the ovaries has many other functions apart from its actions on the uterine lining.
Loss of the ovaries brings on the symptoms of the menopause (see below) and causes bone loss, increasing the risk of osteoporosis in later life. It also causes thinnning and dryness of the vaginal walls, making sexual intercourse painful. If you decide to keep your ovaries after the uterus is removed, the ovaries will continue to produce the same amount of oestrogen for the remainder of their natural lifespan. It is sometimes stated that the ovaries fail earlier after a hysterectomy but recent research has not confirmed this.
Symptoms after ovary removal
Symptoms such as hot flushes, night sweats, vaginal dryness and occasionally mood disturbances may start abruptly after removal of the ovaries. These symptoms vary in severity from woman to woman; some scarcely notice them whereas others are severely troubled for months or even years. However, onset of these symptoms can be prevented by the use of hormone replacement therapy (see below).
Hormone replacement therapy (HRT)
If your ovaries have been removed, oestrogen can be prescribed by your doctor in the form of hormone replacement therapy (HRT). There are many different types of HRT, available as tablets, skin patches or skin gel. It is sometimes given as an implant (a small pellet inserted under the skin), although there are disadvantages to this method and some doctors do not use it. Unlike women prescribed HRT who still have a uterus, women who have had a hysterectomy normally need only one of the two hormones normally produced by the ovaries (oestrogen but not progesterone).
Is HRT suitable for everyone?
As HRT is designed to replace hormones normally produced by the ovaries, it is suitable for most women . However, if you have had treatment for breast cancer or are having a hysterectomy for uterine lining cancer (endometrial cancer), it is not advisable to take HRT. It is also not suitable for women with a strong history of thrombosis (blood clots) or heart disease.
There are some medical conditions for which additional health checks are required if HRT is taken. The most common of these is high blood pressure. However, as HRT has to be prescribed by a doctor, you will be asked a series of questions about your health before HRT is prescribed and this will give an opportunity to raise any concerns that you may have.
Does HRT have any side effects?
Side effects may occur with HRT but most of these are similar to the symptoms that women often experience along with their monthly cycle. The most common are sore breasts, headaches, bloating and fluid retention, but it is unlikely that you would experience all of these. Side effects can often be relieved by prescribing a lower dose of HRT or trying a different preparation.
HRT may cause bleeding problems but this is not relevant if you are taking HRT after a hysterectomy. The main concern raised by women starting HRT is whether they will gain weight. Again this varies and HRT can certainly aggravate an existing weight problem. Any initial weight gain is temporary when you first start HRT and does not usually continue.
What about the risks of HRT?
Women are naturally concerned about potential risks with HRT. On balance, it is felt that the health benefits of HRT outweigh any risks for women who have their ovaries removed before the natural menopause. Not only does HRT treat menopausal symptoms such as sweats and vaginal dryness, and improves the way that you feel, it also protects against bone loss and osteoporosis.
The main disadvantage of taking HRT is that there is an increased risk of breast cancer. However, this risk applies only to women who start taking HRT over the age of the natural menopause (around 50) and take it for five years or more. If you start HRT in your 30s or 40s, it is normally recommended that you take it until you reach the age of 50. HRT causes a slight increase in the risk of venous thrombosis (blood clots in the leg veins) and also increases the risk of heart disease and stroke.
However, these risks apply mainly if you are already at higher risk – for example, if you are overweight or have high blood pressure. Women who are not suitable for HRT patches or tablets may be able to use oestrogen pessaries or cream for the relief of vaginal dryness or painful intercourse. All women are individuals and have different concerns and health factors. It is helpful to discuss the subject with a doctor who is interested in the menopause. For more information readers are referred to the companion booklet in this series, Understanding the Menopause & HRT.
Ovarian disease
If your ovaries are diseased, this may be the major reason for the hysterectomy operation. For example, if you have severe endometriosis or if ovarian cancer is suspected, the best treatment is removal of the uterus and both ovaries.
The other main reason why gynaecologists recommend removal of the ovaries is to prevent the later development of ovarian cancer. This is a very serious condition that is hard to treat, although it is not common.
Some women are at increased risk of developing ovarian cancer because they have a strong family history of this condition. You may also be at increased risk if you have no children, have never been on the oral contraceptive pill or have a history of infertility. If you have concerns about any of these factors you should discuss them with the gynaecologist.
Removal of healthy ovaries
If the reason for your hysterectomy is heavy menstrual bleeding or fibroids and your ovaries are healthy, removing them is not a necessary part of your treatment. Few gynaecologists would suggest doing so if you are under the age of 45 because it is generally believed that the disadvantages outweigh the advantages.
If you are already menopausal or very near the menopause, it may be suggested that you should have your ovaries removed, even if they are healthy, on the basis that they are no longer functioning adequately. However, the decline in hormone production during the natural menopause is much more gradual than the sudden fall that occurs after surgical removal of the ovaries. If you decide to have your ovaries removed you should be well informed about HRT and feel happy about taking it.
If you suffer from severe PMS or PMT, removal of both your ovaries may be recommended on the basis that the symptoms are triggered by the hormonal changes of the menstrual cycle. However, this is a particularly drastic approach to the problem and does not always work. Even worse, you may then find that HRT does not suit you.
By giving a course of medical treatment that stops the production of hormones from the ovaries (a GnRH analogue – see earlier chapter) and then later adding in some HRT, it should be possible to predict which women may benefit from removal of their ovaries.
When should HRT be started?
After a hysterectomy with removal of the ovaries, the symptoms of sudden hormone loss may start almost immediately, although they may be masked by other changes related to the operation. Feelings of being very hot and sweaty may be confused with symptoms of a fever and changes in mood with the stress of surgery.
Hormone lack may contribute to feelings of anxiety and low mood after the operation, and thus there are advantages in starting HRT early on in order to prevent these symptoms. This should not be before you are fully mobile – usually around the time that you are due to be discharged home. The HRT may be supplied by the hospital or you can arrange for your GP to do this.
There may be medical reasons for delaying the start of HRT or you may prefer to wait and see whether you really need it. Not everyone experiences symptoms after removal of their ovaries and the symptoms may be milder if you are already going through the menopause anyway. However, if you are under 45 or have additional risk factors for developing osteoporosis in later life, HRT is usually recommended. If wish to discuss HRT in more detail, ask your GP for advice and look out for leaflets which are available in surgeries and hospital clinics. You’ll find more information about HRT in the companion booklet in this series (Understanding the Menopause & HRT).
What type of HRT should you be taking?
As indicated above, after a hysterectomy HRT containing only oestrogen is usually prescribed. You would need to take combined HRT which also contains progesterone if you have had endometrial ablation because some remnants of the uterine lining usually remain.
Combined HRT is also recommended after a subtotal hysterectomy because the upper cervix may contain uterine lining tissue. Some women who have had a hysterectomy with removal of their ovaries for the treatment of severe endometriosis require progesterone along with oestrogen to ensure that there is no reactivation of any small areas of endometriosis which may still remain. This will be discussed with you before you are discharged from hospital.
Hysterectomy and your menopause
The term ‘menopause’ is used to describe natural failure of the ovaries and you know it has happened when your periods stop. For those who no longer have a uterus, this change is rather meaningless because you are no longer having periods, so there is no easily recognised sign that your ovaries have stopped functioning. It used to be said that ovaries fail earlier after a hysterectomy but this has been disproved by recent research.
You will most probably become aware that you are going through the menopause because you start to experience symptoms such as hot flushes or night sweats. If you are in any doubt, it can be confirmed by measurement of hormone levels in your blood. You can then discuss the need for HRT with your doctor.
KEY POINTS
-
Removal of the ovaries is not an automatic part of a hysterectomy and may have serious implications for future health
-
The hormone oestrogen, produced by the ovaries, has an important function in preserving the health of the bones and vagina
-
Recent research has shown that, if ovaries are left behind, they do not fail any sooner after a hysterectomy
-
If the ovaries have to be removed, hormone replacement therapy (HRT) is suitable for most women
-
HRT can be taken as tablets, skin patches or implants under the skin