Complications after a stroke
Strokes affect many older people, and other common medical conditions, such as heart disease, diabetes or arthritis, are often associated with a stroke. In addition, there are a few conditions that complicate recovery after having a stroke. These are some of the more common problems encountered.
DEPRESSION
Depression is quite common after a stroke, and affects about a fifth of people in the recovery phase. A stroke is a shock to the system and many people suffer losses (for example, of mobility and independence) as a result. The person may need to be admitted to hospital, which can be upsetting, and many patients find that their whole life is totally transformed by the stroke event. Feelings of depression are a natural reaction to this, and sometimes the depression becomes severe enough to need treatment.
The symptoms of depression include low mood, crying, low self-esteem and feelings of hopelessness. Sometimes, depression can affect the appetite, and people simply cannot be bothered to prepare food or eat it. Many of these symptoms, when mild, are a normal part of life, but, when severe, they can cause misery and stop or slow recovery. There is no clear dividing line between low mood and depression, and the doctor will often judge when the symptoms will benefit from treatment with an antidepressant drug. Many different types of antidepressants are available, but the treatment takes time to start working (perhaps two to three weeks) and needs to be continued for months (six months or more). Support from the stroke team is also important for people with depression.
EMOTIONAL CHANGES
Many people experience a change in their emotions after a stroke, because the emotional centres of their brain may have been affected, or the changes that they have experienced may upset them. Some people find that they suddenly burst into tears for no apparent reason, and this type of reaction can continue for several weeks or months and occasionally longer. If this tearfulness is associated with depression, it should respond to antidepressants and, even in the absence of depression, this type of drug can help if the reaction causes distress.
EPILEPSY
Epilepsy is an excessive electrical activity of brain cells that triggers a seizure. Seizures can vary from short lapses in consciousness to severe spasms of the whole body, and some people develop more than one type of fit. A stroke is the most common cause of epilepsy occurring for the first time in older people. It is thought to occur as a result of damage to electrical circuits in the brain or the formation of scar tissue. About five per cent (one in twenty) of patients will have an epileptic fit after a stroke. These fits may require treatment, especially if they recur.
CHEST INFECTIONS
Chest infections can occur after a stroke, especially if the swallow mechanism has been affected. This makes inhalation of food particles more likely, so that inflammation and infections occur. Symptoms include a cough, a high temperature and breathlessness. Most chest infections can be treated with a simple course of antibiotics. Chest physiotherapy and breathing exercises are also helpful.
URINARY TRACT INFECTIONS
A stroke may affect the ability to pass urine, so that the bladder does not empty fully, making infections more common. Stinging or scalding on passing urine may occur, but often the infections go unnoticed by the patient. A short course of antibiotics can treat a urine infection, and nursing care together with good hygiene can reduce the chance of it recurring.
PAINFUL SHOULDER
The shoulder joint is only as strong as its surrounding muscles. These muscles are often weak after a stroke, and the tendons and muscles are easily damaged. Pain may occur in the first few hours and days after a stroke through lying awkwardly, when trying to move about or through accidents such as a fall. Skilled handling by physiotherapists, occupational therapists and nursing staff can often prevent this distressing problem and, if it occurs, physical treatments (provided by physiotherapists) are often better than pain-killers prescribed by doctors.
DEMENTIA
Stroke disease is the second most common cause of dementia after Alzheimer’s disease. This is particularly important if patients have had a number of strokes. Although problems with memory and the intellect after stroke have been recognised for many years, this area has been neglected by many doctors and researchers. Specialists for elderly people (geriatricians) and psychiatrists for elderly people (psychogeriatricians) may be able to provide advice on management and access to local services such as a day hospital or respite support. Occasionally, a stroke can cause very abnormal behaviour, which requires specialised psychiatric nursing and medical care, and medication to control difficult behaviour.
PAIN
Sometimes the stroke affects the pain pathways in the brain, and pain becomes a problem. The pain is often described as being a ‘deep’ pain, a ‘toothache-type pain’ in the bones and muscles of the arm or leg. It tends to follow the same pattern as the weakness after stroke (see ‘Types of strokes’, page 11). This type of pain is often difficult to treat, but various painkillers are available to give some relief.
Case history
A 60-year-old man had a stroke causing a weakness down his left arm and left leg. As the weakness improved, he developed a deep pain in his arm and thigh. Simple pain-killers didn’t help and, after several weeks of discomfort, the doctors found a tablet that took the edge off the pain. This treatment was not a normal pain-killer. It was a drug usually used for epilepsy that seems to dampen down the way that electrical pain messages are passed along nerves.
THROMBOSIS
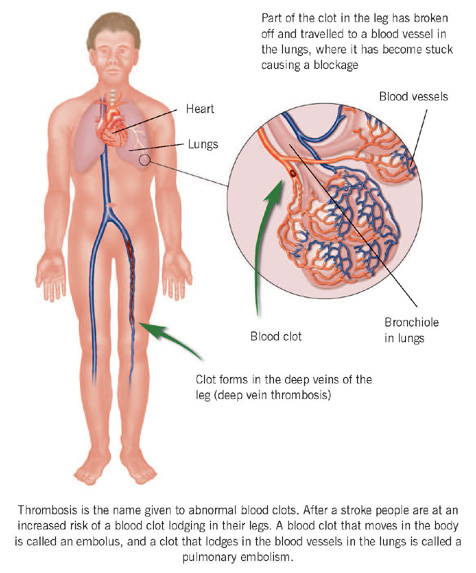
Thrombosis is the name given to abnormal blood clots. After a stroke, people are at an increased risk of a blood clot lodging in their leg (deep vein thrombosis). Movement is important to keep the blood flowing through the leg muscles properly. After a stroke, immobility means that the blood flow through the legs is more sluggish than usual, so clots are more likely to form.
Less commonly, a blood clot can travel from where it formed in the deep veins to obstruct the blood flow in the lungs. This type of wandering blood clot is called an embolus, and a clot lodging in the lungs is known as a pulmonary embolism (pulmonary is the medical word relating to the lungs).
A pulmonary embolism can be a serious complication and may be fatal, because it can prevent enough blood reaching the lungs to receive all the oxygen that the body needs. Fortunately, this is rare, and the rate of a fatal lung thrombosis is probably less than one in a 100 of those with disabling stroke. The symptoms of a pulmonary embolism include sudden breathlessness, palpitations, faintness and chest pain on breathing.
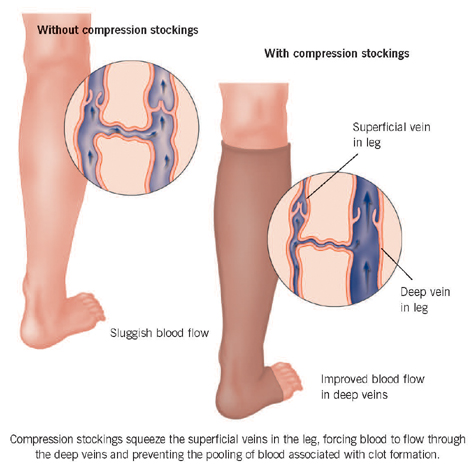
Researchers suspect that deep vein thrombosis and embolism are becoming less common with the modern emphasis on early rehabilitation and early mobilisation after a stroke. Blood-thinning treatments, such as aspirin and heparin, can be life-saving as they thin the blood and help to dissolve the clot. However, although heparin can reduce the chance of developing a leg thrombosis, it can increase the chance of abnormal bleeding in the brain. Other methods of preventing leg thrombosis include special elastic leg stockings, which stop blood pooling in the legs and prevent swelling.
DYING AFTER A STROKE
A stroke is the third most common cause of death in the UK. This is mainly as a result of a stroke affecting older people, many of whom already have other serious medical problems. After a stroke, about 10 per cent of people (one in 10) die within a week, 20 per cent within a month and 30 per cent within a year. About a fifth of people admitted to hospital will die as a direct result of their stroke.
Most people die very peacefully after a major stroke and are not in any pain or discomfort. Some strokes are so severe that they cause immediate coma. Death occurs when the brain is no longer able to keep the body breathing or the circulation flowing. This results from the effect of the stroke on a part of the brain called the brain stem, which means that the person drifts into a deeper and deeper coma and eventually dies.
Occasionally, people survive in a coma for a few weeks (or even longer), and this period can be very distressing for the family and stroke team. There is often the dilemma of what to do about feeding the patient. Some patients appear more comfortable without feeding tubes or intravenous or subcutaneous drips. But some families become very distressed at the thought of not feeding someone and, of course, this will always lead to death. If there is genuine uncertainty about the degree of recovery, it is often wiser to continue some fluid and nutritional support. There are no easy answers, and it is often best to discuss these issues with the stroke team.
If the stroke has caused so much brain damage that the patient has been in a coma for more than a few days, they may not recover and the treatment should aim to keep them comfortable. Good nursing care is required, ideally in a quiet, well-lit environment with privacy for the family. Sometimes, giving the patient fluid (via a drip) can appear to help, but on other occasions this treatment can cause swelling (oedema) of the legs and arms. The question of whether to give fluid will therefore depend on the state of the patient and avoiding fluids can actually be a positive decision. Despite good nursing care and nutritional support, most patients in coma following stroke die within days or weeks of their stroke.
Deaths after a stroke are often not the result of the direct effects of the stroke on the brain but of the complications of becoming disabled. These complications include chest or urinary infections and thrombosis affecting the lungs (pulmonary embolism).
‘DO NOT RESUSCITATE’ ORDERS
If someone is admitted to hospital after a stroke, there is usually a cardiac resuscitation team in the hospital to try to save lives in the event of a cardiac or respiratory arrest (when the heart or breathing stops). Unfortunately, the success rate is not good for many patients and prolonged resuscitation often causes brain damage. Doctors may decide that resuscitation is so unlikely to succeed that it is best avoided for some people. In this situation, they may recommend a ‘Do not resuscitate’ order. If the doctors feel that a patient may benefit from resuscitation, the patient may be asked for their views on this. Some people do not want resuscitation and have strongly held views on the matter. Do not be alarmed if this subject is mentioned during the hospital stay, because it is increasingly common to obtain the views of patients and relatives on these difficult ethical decisions.