Why can’t we conceive?
ELEMENT OF CHANCE
Most couples have unrealistically high expectations of how quickly they will conceive when they start trying for a family. For normal fertile couples, the monthly chance of conception varies between one in three (at the most) and about one in twenty, the average being about one in six. Many couples find it difficult to accept that chance has anything to do with achieving a pregnancy and that their failure to conceive may simply be the result of bad luck.
If we take the example of an average fertile couple with about a one in six monthly chance of pregnancy, we can compare this to the frustration of repeatedly failing to throw a six with a dice. The dice is not weighted against us, we are simply being unlucky. Of course, the more times a dice is thrown for a six unsuccessfully, the more likely it becomes that there is a problem with the dice – that it is weighted against us. Or, in the case of pregnancy, that there is a fundamental problem reducing the chance of conception.
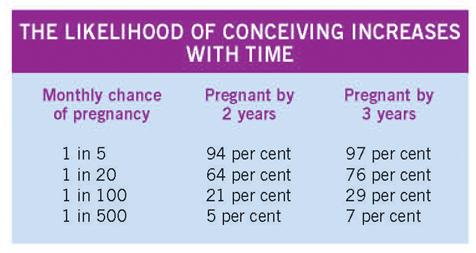
A couple throwing a 20-sided dice for a ‘20’ is roughly equivalent to the lower limit of normal human fertility. For such a couple with low fertility, after 24 throws, or two years of trying, there is about a 65 per cent chance of success, which increases to about 75 per cent after 36 throws or three years of trying. Very few couples have a zero chance of pregnancy and, even with a very small chance each month, it is possible that they will conceive in time. For example, even with a one in 100 chance each month, almost 30 per cent of couples would have achieved a pregnancy by three years.
For most infertile couples, their chance of conceiving naturally is likely to be unrealistically low by the time they are seen in a specialist clinic. Depending on whether a fertility problem is found and of what type, there are likely to be a number of options for treatment. Each treatment is likely to offer a different chance of success, but it is unreasonable to expect any of them to exceed the highest monthly chance for couples with normal fertility: about 33 per cent (one in three).
IS OVULATION OCCURRING?
If you have a regular monthly period (never more than one or two days early or late), you will almost always be releasing an egg from one of your ovaries. This usually occurs about 14 days before your period would be due to start. Many women are able to recognise the time of ovulation – they may experience low abdominal discomfort for a few hours on the side where an egg has just been released or may notice an increased amount of mucus discharge from their vagina for a day or two beforehand. Women who have irregular or infrequent periods are likely to have a reduced chance of conceiving, and many may not be ovulating at all.
If your periods have been very regular in the past and have only become irregular fairly recently, this may be caused by being underweight, losing weight rapidly through dieting, emotional stress or too much exercise. Changing your lifestyle may be all that is necessary to correct this.
If your periods have always been irregular, or have become irregular with a steady increase in weight, you may have a condition called polycystic ovarian syndrome (PCOS). This is an inherited condition that can cause subfertility, irregular periods and possibly increase the risk of miscarriage. In PCOS, the ovaries contain many small benign (non-cancerous) cysts. The cysts are actually immature egg follicles and not true ‘cysts’. They do not usually need to be removed by surgery, although this may be necessary if a large cyst develops.
PCOS causes a hormone imbalance, which can result in irregular ovulation, failure of ovulation, or a reduction in the quality of eggs that the woman releases from her ovaries. Other symptoms include an increased tendency to develop acne, an increased amount of body hair, an increased tendency to put on weight and difficulty in losing weight. Many women with PCOS need medical treatment. However, some find that by losing weight their menstrual cycle becomes more regular. This improves their chance of conception and reduces their risk of miscarriage. It may often help their other symptoms.
TIMING AND FREQUENCY OF INTERCOURSE
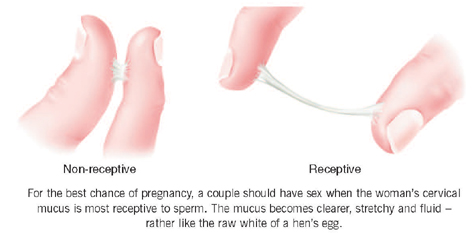
For the best chance of pregnancy, a couple should have sexual intercourse when the woman’s cervical mucus is most receptive to sperm, usually one or two days before ovulation. Most women are aware that they produce more cervical mucus in the middle of their cycle. Their cervical mucus becomes clearer in appearance and more stretchy and fluid, rather like the raw white of a hen’s egg. Some women will notice that they feel more damp at this time. A woman’s sex drive may also be noticeably increased, as a result of hormonal changes around the time of ovulation. Some couples use commercially available ovulation detection kits, which identify these hormone changes, to determine when the woman is ovulating. We do not consider that these kits add to the chance of conception when used by women with regular cycles, those who recognise their cervical mucus, or both.
It is not necessary for couples to focus their love-making solely around the time of ovulation. This can lead to difficulties in a couple’s relationship, as both partners may start to feel that they are having to perform to a schedule. The timing of intercourse is not particularly critical if a couple are having intercourse every two to four days. Once in the cervical mucus, sperm can survive for several days, possibly up to a week, and will retain their normal ability to fertilise an egg for most of this time. They gradually pass through the cervical mucus into the woman’s uterus and along her fallopian tubes where, if they meet the egg, fertilisation normally occurs.
There is no evidence that a couple’s chance of pregnancy is reduced by having intercourse too often. Although the volume of semen a man releases may be less, this is simply the result of a reduction in the fluid content. The number of functionally competent sperm remains virtually unchanged. There is also no evidence that the position of sexual intercourse makes pregnancy more or less likely. Neither does lying still for any period of time after sex or propping a pillow under the buttocks.
LIFESTYLE FACTORS
A number of lifestyle factors and past or current medical problems may reduce your chance of pregnancy. The main lifestyle factors to consider are smoking and alcohol.
Substances in cigarette smoke are toxic to eggs and sperm, and to the developing embryo in pregnancy. Smoking by either partner reduces the chance of getting pregnant naturally or by fertility treatments, and there is increasing evidence that passive exposure to cigarette smoke may be almost as harmful. Smokers take about 30 per cent longer to achieve a pregnancy than non-smokers and, with IVF treatment, the proportion of eggs that fertilise will be 20 to 30 per cent lower. You should try to give up smoking while you are at an early stage of infertility investigations.
Heavy alcohol consumption can affect important hormone levels in men and women, and interfere with sperm production and sperm function. However, smaller amounts of alcohol do not seem to be damaging. It is sensible for you both to restrict your alcohol consumption to less than six units each week while you are trying for a pregnancy (one unit is equivalent to a half-pint of beer or a small glass of wine).
The effect of being under- or overweight
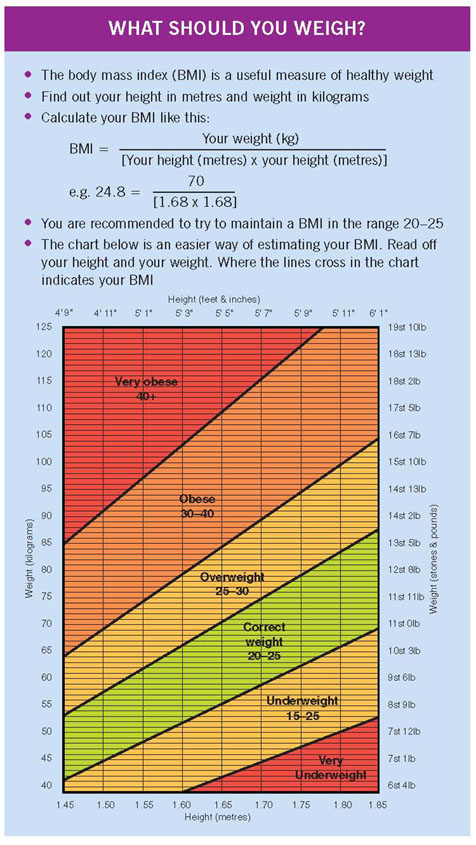
A woman’s weight has an effect on the likelihood of her conceiving and the likelihood of her having an uneventful pregnancy. The relationship between height and weight is usually calculated as a body mass index (BMI). This is calculated by a formula in which the body weight (in kilograms) is divided by the height of the person (in metres) squared, that is, kilograms/metres2. This means that, for somebody whose body weight is 50 kilograms and height is 1.4 metres, the BMI is calculated as 50 divided by the square of 1.4 (50/1.96), approximately 25. The normal range of BMI is 20 to 25. There are also charts available that allow calculation of the BMI without the need to go through this formula (see the box).

Women whose BMI is less than 20, or more than 25, have a reduced chance of conception, and the greater the increase beyond 25, the more severe the effect on the chance of pregnancy. A raised BMI is also associated with an increased risk of miscarriage. It is therefore in a woman’s best interest to lose weight if she has a BMI greater than 25 and is having difficulty in conceiving (see figure).
Not only does being overweight or underweight have effects on getting pregnant; there are further effects on the outcome of the pregnancy itself. Women who are overweight are much more likely to encounter the following pregnancy complications: caesarean section, diabetes in pregnancy, very big babies (which is not a good thing), high blood pressure and pre-eclampsia (toxaemia) and excessive bleeding or infection after delivery.
In women who are underweight, anaemia in pregnancy, pre-term delivery and having a very small baby are more likely to occur than in women of normal BMI.
MEDICAL PROBLEMS
If you have experienced medical problems in the past, this can reduce your chance of getting pregnant, so seek advice early on. For the man, this may be because of a testicular infection (orchitis) or surgery in the past. Orchitis is most likely to damage sperm production if it is caused by a viral infection such as mumps. If it is caused by a bacterial infection, it may lead to scarring and obstruction of the vas deferens and epididymis. Previous surgery in the area around the testes can also damage these narrow tubes or restrict the blood circulation to the testes. Operations for childhood hernias, to correct any failure of the testes to descend properly into the scrotum or to treat the painful emergency of testicular torsion, are important indications to seek fertility advice early.
For the woman, any past gynaecological problems or pelvic infection may affect her fertility, as well as any previous pelvic or abdominal operations. Surgery causes scar tissue to form as part of the normal healing process and sometimes other tissues close by can be involved. For example, the fallopian tubes may become obstructed by scar tissue after severe appendicitis or surgery to remove an ovarian cyst.
Current medical problems may also reduce your fertility. Some of these (such as thyroid disease) are checked for during routine fertility investigations. For other medical conditions, such as diabetes or epilepsy, you may need to have an assessment before you try for a pregnancy. If in doubt, see your GP.
THE EFFECT OF MEDICATION
Various drugs can reduce your fertility. If you are taking medicines regularly, check with your GP, pharmacist or local fertility clinic before trying for a pregnancy. As a general rule, it is best to avoid all drugs that are not absolutely necessary while trying to conceive.
Drugs that can affect a man’s fertility include sulphasalazine, which is used in the treatment of inflammatory bowel diseases, and some blood pressure treatments, such as beta-blockers and captopril (which can also cause impotence). Anti-malarial drugs may reduce sperm counts, as can the excessive use of simple pain-killers such as aspirin. Drug abuse can also reduce male fertility, particularly anabolic (‘body-building’) steroids and marijuana.
Drugs that reduce a woman’s fertility usually do so by interfering with ovulation. Some affect a woman’s normal hormone levels by increasing the production of the hormone prolactin. Although prolactin is an important hormone for the production of breast milk after pregnancy, it stops a woman having periods if she produces it excessively at other times. Drugs that can cause excessive prolactin production include various tranquillisers, sedatives and other treatments for minor psychiatric problems, as well as some anti-sickness drugs such as metoclopramide. A wide range of anti-inflammatory drugs and anti-arthritis drugs can reduce a woman’s fertility by blocking ovulation. Examples of these are indomethacin, naproxen, diclofenac and mefenamic acid. Even aspirin or paracetamol can cause problems if they are taken in high doses. As in men, drug abuse will also reduce a woman’s fertility, particularly marijuana, which can suppress the hormones follicle-stimulating hormone (FSH) and luteinising hormone (LH).